
What is Knee Osteoarthritis?
Managing Osteoarthritis: What you need to know.
21 October 2025
Introduction Osteoarthritis: A Growing Global Challenge
Osteoarthritis (OA) is the most common form of arthritis worldwide, affecting an estimated 528 million people — around 3.3–3.6% of the global population. With people living longer and staying active later in life, these numbers are only expected to rise in the coming decades.
The Scale of the Problem
OA most frequently affects the knee joint, a key area of focus for physiotherapists. It’s estimated that around 250 million people globally live with knee osteoarthritis, making it one of the leading causes of pain and disability in older adults.
In the UK alone, nearly one in five people over the age of 45 have sought treatment for knee OA, a statistic that highlights the growing demand for effective rehabilitation and management strategies.
What is Knee Osteoarthritis (Age-Related Knee Pain)?
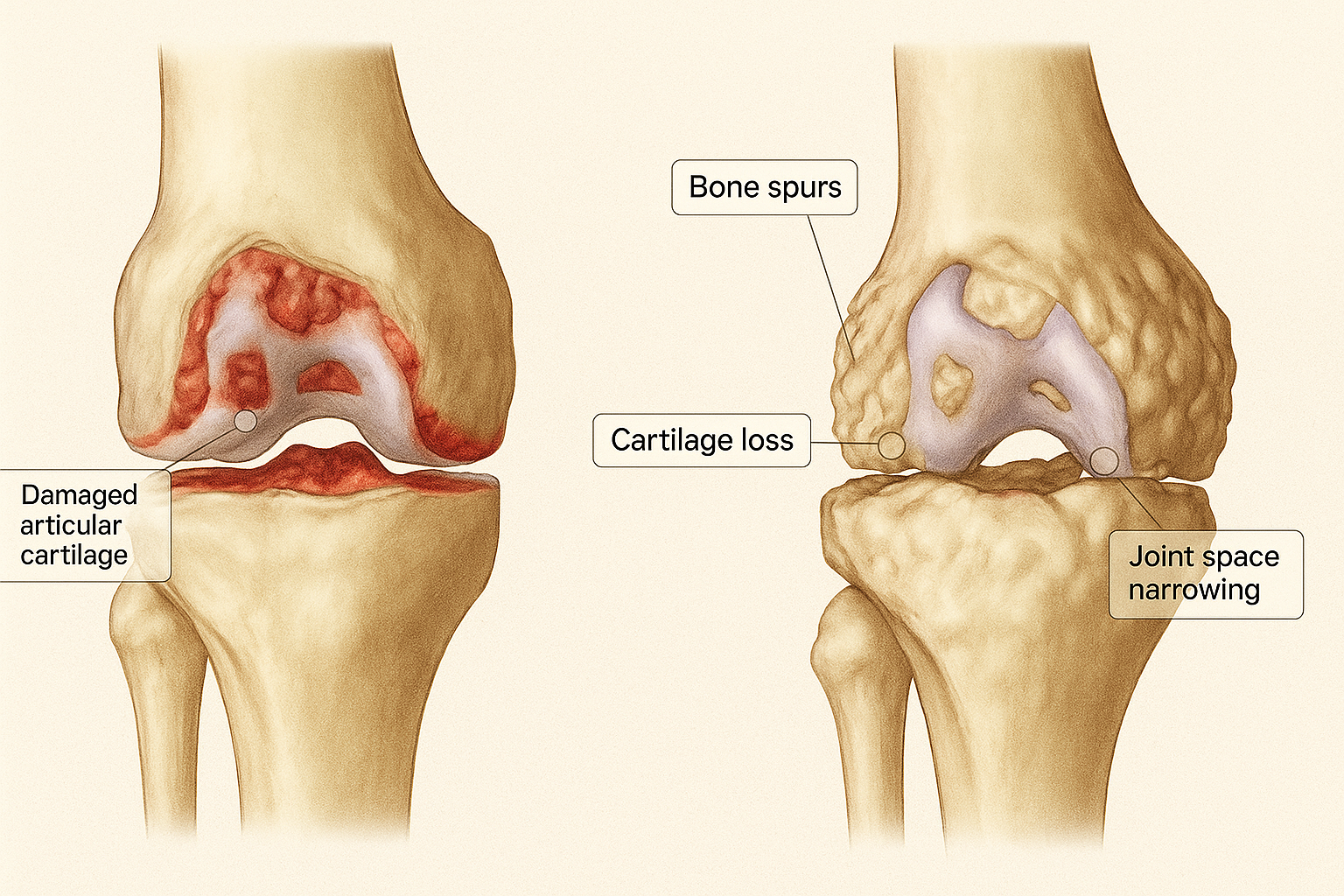
Knee osteoarthritis (OA) is a common, age-related condition that affects the structure and function of the knee joint. As we get older, it's normal for our joints to go through changes, and osteoarthritis is part of this natural ageing process.
In osteoarthritis, the smooth cartilage that covers the ends of the bones begins to wear down. This cartilage acts as a cushion, so when it becomes thinner, it can lead to increased friction in the joint. Over time, the body may respond by forming small bony growths known as osteophytes, and the synovial fluid—which normally lubricates the joint—can also change, contributing to joint stiffness. In some cases, the space between the bones may narrow, further limiting movement.
These changes are partly due to low-level inflammation and partly your body’s way of trying to repair and adapt to the wear and tear. While this is a natural process, it tends to occur sooner and more noticeably in joints that bear weight, such as the knee and hip.
It's important to note that many people with knee osteoarthritis experience no pain at all. However, as the condition progresses, it can lead to increasing stiffness, discomfort, and reduced mobility—especially during or after activity.

Understanding the Anatomy of the Knee
The knee is one of the largest and most complex joints in the body. Acting like a hinge, it allows for bending and straightening while also withstanding a significant amount of twisting and turning during daily activities. Whether you're walking, climbing stairs, or playing sports, a strong and stable knee is essential for movement and performance.
Bones The knee joint is formed by three main bones:
The femur (thigh bone)
The tibia (the larger of the two shin bones)
The patella (kneecap)
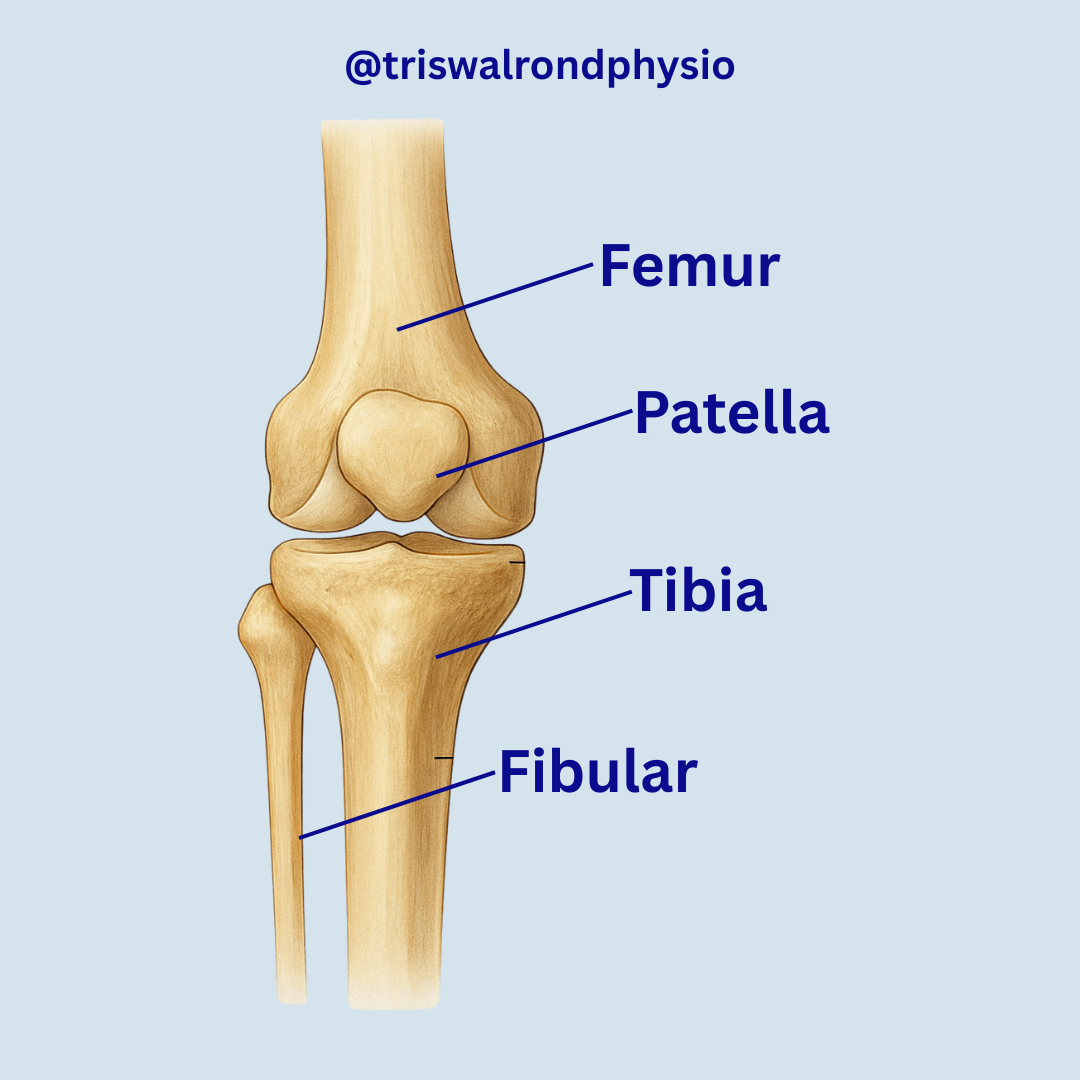
While the smaller shin bone—the fibula—sits nearby and plays a supporting role, it is not directly involved in forming the knee joint itself.
Ligaments The knee is stabilized by four strong ligaments:
On the outside of the joint: the medial collateral ligament (MCL) and lateral collateral ligament (LCL)
Inside the joint: the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL)
These ligaments help keep the knee stable and aligned during movement.
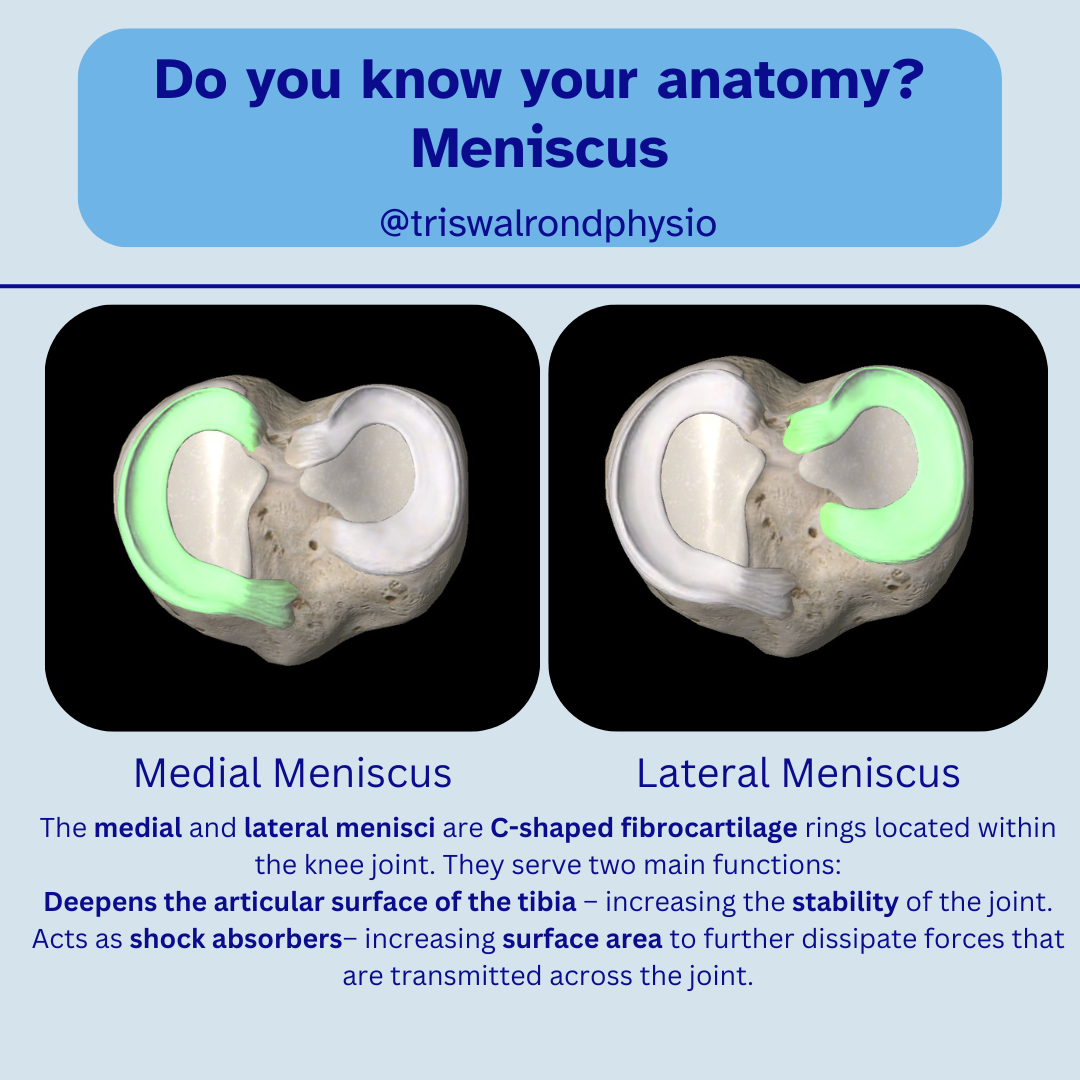
Cartilage (Menisci) Within the knee are two crescent-shaped pieces of cartilage called the menisci. These act as shock absorbers and contribute to joint stability by cushioning the space between the femur and tibia.
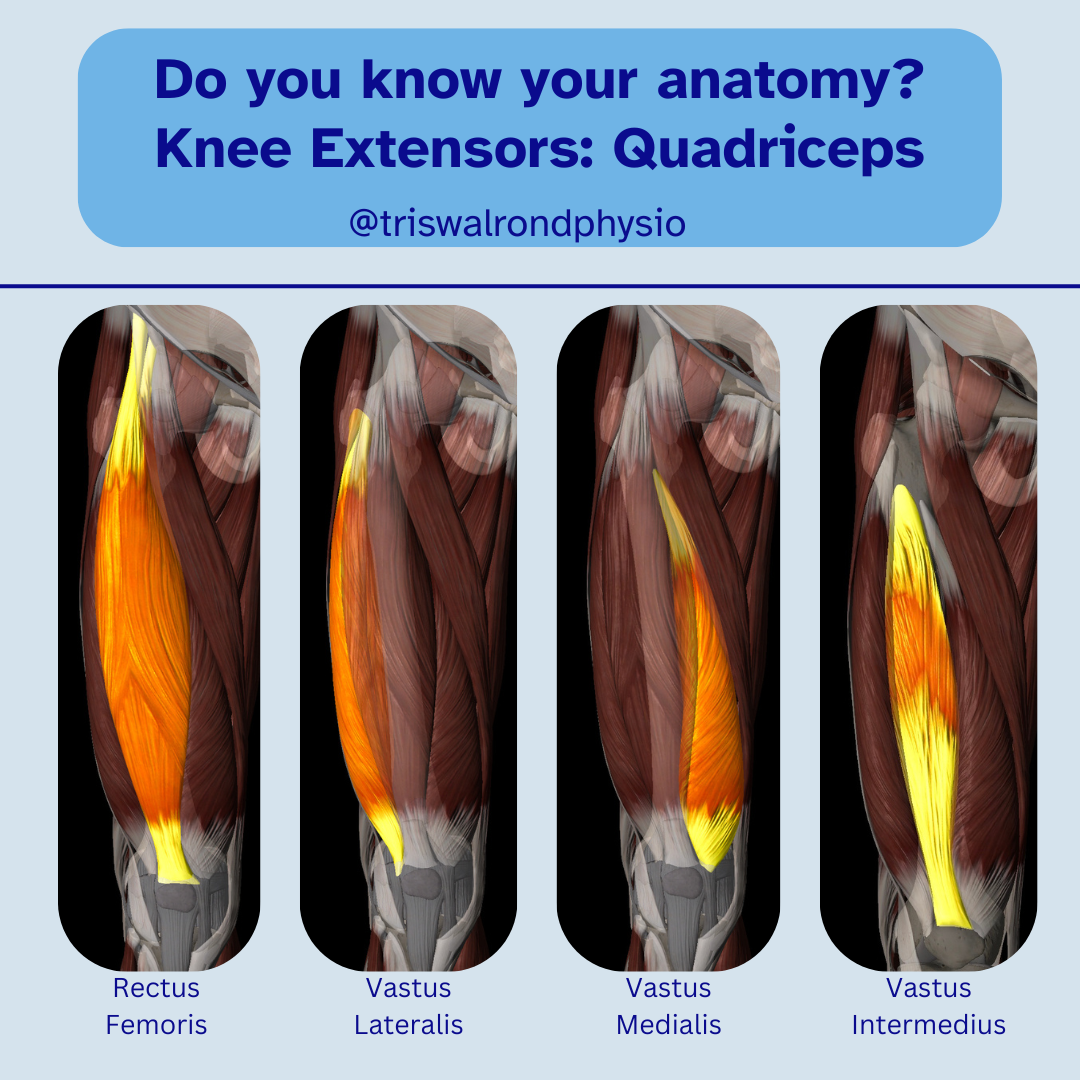
Muscles Muscles that cross the knee provide movement and additional support. They attach to bones via strong connective tissues called tendons, and play a key role in absorbing forces placed on the joint. The main muscle groups involved are:
The quadriceps (front of the thigh)
The hamstrings (back of the thigh)

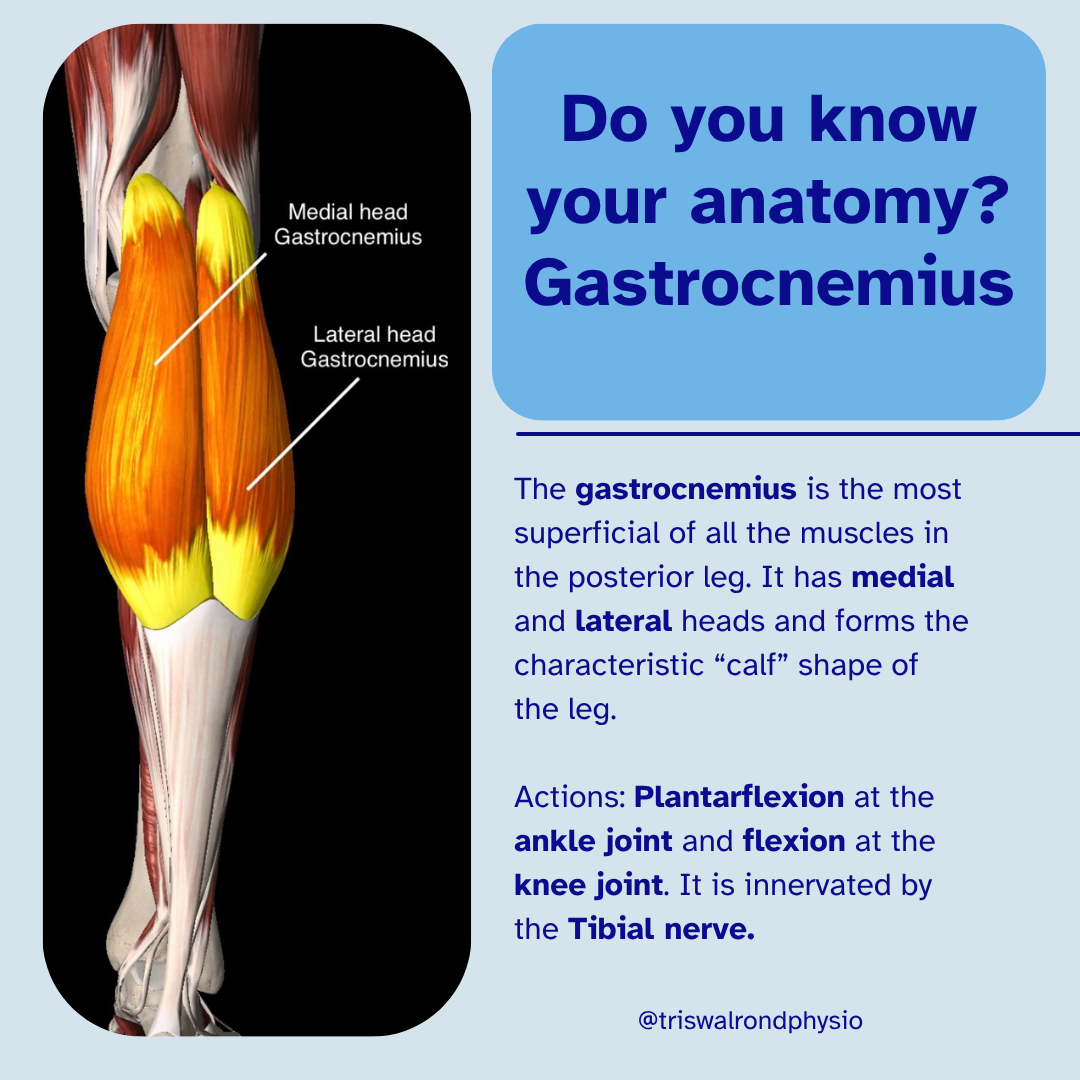
The gastrocnemius and soleus (calf muscles)
Joint Capsule and Synovial Fluid The knee joint is enclosed in a capsule filled with synovial fluid, which lubricates the joint and reduces friction during movement. Regular movement helps distribute this fluid across joint surfaces—explaining why we often feel stiff after sitting still for too long.
Symptoms of Osteoarthritis
Osteoarthritis (OA) of the knee can develop gradually, with symptoms varying in severity from person to person. The condition often affects people over the age of 45, and symptoms typically worsen with activity or after prolonged periods of rest.
Common symptoms include:
Pain: Usually worsens with movement or weight-bearing activities such as walking, climbing stairs, or standing up after sitting for a long time.
Stiffness: Especially noticeable after rest or in the morning, typically lasting less than 30 minutes.
Swelling: This may feel hard due to bony changes or soft from fluid build-up within the joint.
Grinding or grating sensation (crepitus): You may feel or hear a grinding noise when moving the knee.
Reduced range of motion: Bending or straightening the knee can become limited over time.
Weakness or muscle wasting: The quadriceps muscles at the front of the thigh can weaken due to reduced activity.
Joint instability: The knee may occasionally “give way” or feel as though it could lock during movement.
Difficulty with daily activities: Tasks such as going up or down stairs, kneeling, or squatting may become painful or challenging.
Altered gait or limping: Pain and stiffness can change the way you walk, sometimes leading to limping or loss of balance.
Imaging
According to the NICE guidelines (2020), an X-ray is not always needed to diagnose osteoarthritis (OA). In most cases, your physiotherapist or doctor can make the diagnosis based on your symptoms and a physical examination.
Imaging is usually only recommended if your symptoms are getting worse, not improving with treatment, or if there’s a need for a specialist review (for example, by an orthopaedic surgeon).
What an X-ray Can Show
When an X-ray is taken, it can reveal certain changes that are typical in osteoarthritis. These can be remembered with the simple “LOSS” mnemonic:
L – Loss of joint space: The space between the bones becomes smaller as the smooth cartilage wears down.
O – Osteophytes: These are small bony growths that form around the edges of the joint.
S – Subchondral sclerosis: The bone underneath the cartilage becomes thicker and harder.
S – Subchondral cysts: Small fluid-filled pockets can form inside the bone near the joint.
Management of Osteoarthritis
A Holistic Approach
Managing osteoarthritis (OA) isn’t about one quick fix — it’s about taking a holistic approach that combines education, exercise, lifestyle changes, and, when needed, medical or surgical options.
According to the NICE guidelines (2020), the core treatments for OA include education, exercise, and weight management.
Education
Understanding osteoarthritis is the first step in managing it well.
It’s important to know that OA isn’t just “wear and tear.” That phrase can make it sound like the joint is permanently damaged — which isn’t true. The joint is constantly adapting and trying to repair itself. A more positive way to think of OA is as a “wear and repair” process.
Using the right language helps reduce fear and anxiety and encourages patients to stay active.
📘 Tip: Visit the Versus Arthritis website for helpful information and self-management advice.
Exercise
Exercise is one of the most effective ways to manage OA symptoms. The key is to create a personalised plan that includes:
Mobility and strengthening exercises to keep the joint flexible and muscles strong.
Aerobic exercise such as walking, swimming, or cycling to boost overall fitness and mood.
Regular exercise helps reduce pain, improve function, and support joint health.
Physical Activity & Weight Management
Staying active not only strengthens your joints but also helps manage pain, improve mood, and support healthy weight loss — which can reduce pressure on the knees.
🟢 Check out the WHO Physical Activity Guidelines for recommendations on how much activity to aim for. 🥗 For healthy eating advice, visit the OA and Diet Food Fact Sheet.
Activity Modification & Pacing
Finding the right balance with activity is key — joints need movement and loading to stay healthy, but too much too soon can trigger pain or inflammation.
You can use a traffic light system to guide your activity level:
🔴 Red (7–10/10 pain): You’ve overdone it — reduce intensity or rest. 🟠 Amber (4–6/10 pain): The “sweet spot” — enough to strengthen and stimulate repair without a flare-up. 🟢 Green (1–3/10 pain): Too easy — increase intensity slightly.
Additional Supports & Pain Relief
Other helpful treatments may include:
Pain relief: Over-the-counter options like paracetamol or topical anti-inflammatory gels (NSAIDs) can ease discomfort.
Heat or ice therapy: Applying warmth or cold can help reduce stiffness and pain (NICE, 2014).
Footwear and walking aids: Supportive shoes or a walking stick can reduce stress on the knee joint.
Corticosteroid Injections
In some cases, a steroid injection may be offered. It combines a local anaesthetic with an anti-inflammatory medication and can provide short-term relief (weeks to months). However, repeated injections are not recommended, as they may weaken cartilage over time (Hauser, 2009).
Surgical Management
For some people, surgery may be considered when symptoms of osteoarthritis (OA) remain severe despite trying other treatments such as exercise, physiotherapy, and pain relief.
The decision to have surgery should always be made together with your orthopaedic surgeon, based on how much your pain and stiffness affect your daily activities and quality of life.
The Oxford Knee Score
The Oxford Knee Score is a short questionnaire used to assess your pain and knee function. It helps healthcare professionals understand how your knee symptoms impact your life and whether it may be time to discuss a referral to an orthopaedic specialist.
It’s important to note that this score does not decide whether you need surgery — it’s simply one part of the overall assessment. The final decision should be a shared discussion between you and your surgeon (Robb et al., 2013).
When Surgery May Be Considered
Surgery is usually recommended for people who:
Have not improved with physiotherapy and other conservative treatments.
Experience significant pain or stiffness that limits daily activities, sleep, or mobility.
Have reduced quality of life because of their symptoms.
Types of Knee Surgery
Partial (Unicompartmental) Knee Replacement
This procedure replaces only the damaged part of the knee joint. Benefits include:
Less invasive surgery.
Faster recovery and shorter hospital stay.
However, because only one part of the knee is replaced, some people may later need a revision or total knee replacement if arthritis develops in other parts of the joint.
Total Knee Replacement
This operation replaces the entire knee joint with an artificial implant. It has excellent long-term outcomes and can significantly improve pain, movement, and overall function.
Recovery can take around 12–18 months, so it’s important to stay active and follow your rehabilitation and exercise programme after surgery to achieve the best results.
✅ Key Takeaway: Surgery can be life-changing for people with advanced knee osteoarthritis, but it’s usually considered after other treatments have been tried. Working closely with your healthcare team and staying active before and after surgery can greatly improve your recovery and long-term outcomes.
Book an appointment and see how physiotherapy can help you manage your Knee Osteoarthritis.
References
Hauser (2009) The deterioration of articular cartilage in osteoarthritis by corticosteroid injections, Journal of Prolotherapy, 1(2), pp. 107-123
NICE, (2020). Osteoarthritis: care and management
Robb CA, McBryde CW, Caddy SJ, Thomas AM, Pynsent PB. Oxford scores as a triage tool for lower limb arthroplasty lead to discrimination and health inequalities. The Bulletin of the Royal College of Surgeons of England. 2013 Apr 1;95(4):1-4